Sarcoma
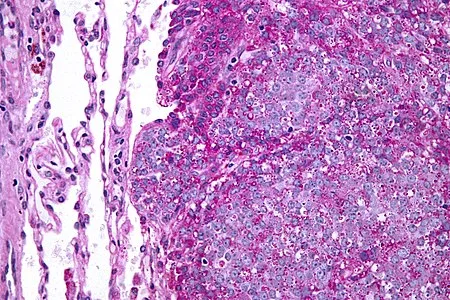
Sarcomas are a heterogeneous group of tumors with more than 80 identified types, that derive from primitive mesenchymal cells, which themselves arise from muscle, connective tissue, supportive tissue and vascular tissue. They account form more than 20% of solid tumors in the pediatric population and young adults, and are the third most common cancer after leukemia and central nervous system tumors (1). The most frequent types in childhood and young adults are rhabdomyosarcoma and Ewing sarcoma.
Standard therapies include surgery, chemotherapy and radiotherapy with different protocols depending on tumor type and stage. When chemotherapy is needed, it often involves the use of high does gonadotoxic agents, resulting in an increased risk of premature ovarian insufficiency in those patients. It is therefore of paramount importance to address young patients diagnosed with sarcoma to fertility preservation, which could be either performed through oocyte cryopreservation in case of in young women, or ovarian tissue cryopreservation in prepubertal patients.
Ovarian involvement has been reported in certain types of sarcoma, including Ewing sarcoma and osteosarcoma, while is extremely rare in rhabdomyosarcoma (2,3). Therefore, it is important to evaluate the presence of malignant cells in cryopreserved ovarian cortical strips, upon ovarian tissue transplantation. Investigations of minimal residual disease in case series of patients who had cryopreserved their ovarian tissue after diagnosis of sarcoma evidenced the possibility of occult malignant cells within ovarian tissue in patients diagnosed with Ewing sarcoma (4,5), while no evidence of minimal residual disease was detected for the other types of sarcoma (6,7).
For this reason, ovarian tissue transplantation in sarcoma patients can be considered safe, except for Ewing sarcoma, in whom caution should be exercised.
References:
- Burningham Z, Hashibe M, Spector L, Schiffman JD. The epidemiology of sarcoma. Clin Sarcoma Res. 2012 Oct 4;2(1):14.
- Eltabbakh GH, Belinson JL, Biscotti CV. Osteosarcoma metastatic to the ovary: a case report and review of the literature. Int J Gynecol Pathol. 1997 Jan;16(1):76-8.
- Sullivan HC, Shulman SC, Olson T, Ricketts R, Oskouei S, Shehata BM. Unusual presentation of metastatic Ewing sarcoma to the ovary in a 13 year-old: a case report and review. Fetal Pediatr Pathol. 2012 Jun;31(3):159-63.
- Abir R, Feinmesser M, Yaniv I, Fisch B, Cohen IJ, Ben-Haroush A, Meirow D, Felz C, Avigad S. Occasional involvement of the ovary in Ewing sarcoma. Hum Reprod. 2010 Jul;25(7):1708-12.
- Yding Andersen C, Ernst E, Bærentzen S, Birkebæk NH, Clausen N. No malignancy detected in surplus ovarian tissue from a former Ewing sarcoma patient who experienced relapse four years after being grafted with frozen/thawed ovarian tissue. J Assist Reprod Genet. 2014 Nov;31(11):1567-8.
- Greve T, Wielenga VT, Grauslund M, Sørensen N, Christiansen DB, Rosendahl M, Yding Andersen C. Ovarian tissue cryopreserved for fertility preservation from patients with Ewing or other sarcomas appear to have no tumour cell contamination. Eur J Cancer. 2013 May;49(8):1932-8.
- Dolmans MM, Iwahara Y, Donnez J, Soares M, Vaerman JL, Amorim CA, Poirel H. Evaluation of minimal disseminated disease in cryopreserved ovarian tissue from bone and soft tissue sarcoma patients. Hum Reprod. 2016 Oct;31(10):2292-302.