Whole ovary cryopreservation



Ovarian cryopreservation and transplantation procedures have so far been almost exclusively limited to avascular cortical fragments, which are grafted without vascular anastomosis and are completely dependent on the establishment of neovascularization after grafting. Consequently, the cells in the graft undergo significant ischemic and reperfusion damage (1) that can induce a high rate of follicular loss (2,3,4). Reducing the ischemic interval between transplantation and revascularization is therefore essential to maintaining the viability and function of the graft. The best way to achieve this would be by transplantation of intact ovary with vascular anastomosis, allowing immediate revascularization of the transplant.
Technique
Whole ovary cryopreservation has been performed on eleven patients in our department to date, using the following technique.
Laparoscopic ovariectomy
A laparoscopy is performed under general anesthesia. The following four laparoscopic puncture sites, including the umbilicus, are used: 10 mm umbilical, 5 mm right, 10 mm medial (allowing the use of 5-mm instruments) and 5 mm left lower quadrant, just above the pubic hairline. Lateral incisions are made next to the deep epigastric vessels. A cannula is placed in the cervix for appropriate uterine mobilization.
After inspection of the whole abdominal cavity, biopsies are taken from the right ovary for cryopreservation of ovarian cortex, according to a protocol described elsewhere (5).
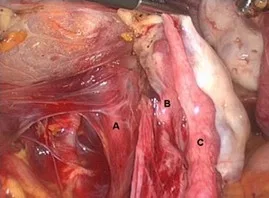
The left ovary then is grasped with atraumatic forceps. The ureter and the iliac vessels are identified. If adhesions are found between the sigmoid and the lateral abdominal wall, they are freed. The broad ligament is incised with scissors from the infundibulopelvic ligament to the round ligament, externally to the fallopian tube (Fig. 1).
Bipolar coagulation is avoided as far as possible. After dissection of the ureter, the posterior part of the broad ligament is opened with scissors. The ovarian pedicle and the ureter are dissected cranially, as high as possible, above the iliac vessels and psoas muscle (Fig. 2). An endobag (Lapsac; Cook, Limerick, Ireland) is introduced through the inferior medial trocar and opened in the pouch of Douglas.
The proximal isthmic part of the fallopian tube and the utero-ovarian ligament are clamped with two vascular clips (Hem-O-Lok; Weck Closure Systems, Research Triangle Park, NC) and cut. The ovarian pedicle is then clamped with three vascular clips and cut between the two proximal clips (Fig. 3).
Care is always taken to place the clips as high as possible on the pedicle, leaving at least 5-6 cm of the vascular pedicle attached to the ovary. The freed ovary and fallopian tube are swiftly placed in the endobag and removed from the abdomen through the medial suprapubic incision, which is slightly extended to avoid damage to the ovary.
The removed ovary is then immediately handed over to a second team present in the operating room, that includes a microsurgeon and biologist.


Ovarian cryopreservation
The ovary is deposited on a sterile Petri dish containing heparinized physiologic solution (100 IU of heparin per mL). The Petri dish itself is placed on a cooling plate at 4°C. The clip on the ovarian pedicle is removed and the pedicle is dissected with microsurgical instruments under stereomicroscopic visualization.
The artery is catheterized with a perfusion catheter, the size of which is determined by the size of the main ovarian artery (range, 24-18G; Fig. 4). The catheter is fixed to the artery with nonresorbable 9-0 sutures. The ovarian artery is perfused with heparinized saline solution.
A precalibrated pump (Terumo Corporation, Tokyo, Japan) is used to maintain a flow rate of 2.5 mL/min, according to the technique described by Martinez-Madrid et al. (6). This perfusion with heparinized physiologic solution continues until the perfusion liquid draining out of the ovarian veins runs clear and all the blood has been evacuated from the ovary, which takes up to 20 minutes.
Thereafter, the ovary is transferred to a second Petri dish and perfused and immersed in a cryoprotective solution of HEPES-MEM (GIBCO, St. Louis, MO), supplemented with 10% dimethyl sulfoxide (Sigma, St. Louis, MO) and 0.4% human serum albumin (Red Cross, Brussels, Belgium) for 5 minutes at 4°C at a flow rate of 2.5 mL/min, as described elsewhere (6).
The ovary is then placed in a cryovial, in which it is pre-equilibrated at 4°C in a bath with the cryoprotectant for 10 minutes. The cryovial is gently shaken while being transferred to the laboratory. After pre-equilibration, it is placed in a 5100 Cryo 1°C Freezing Container (Nalgene; VWR, Belgium) precooled at 4°C, and deposited in a -80°C freezer. This confers a cooling rate of -1°C/min. After 24 hours in the -80°C freezer, the cryovial containing the ovary is transferred to liquid nitrogen (-196°C).
Discussion
Ovarian vascular transplantation has already been successfully performed with intact fresh ovaries in rats (7,8), sheep (9,10), rabbits (11), dogs (12), monkeys (13), and humans (14,15,16). It appears that, in large mammals and human beings, anastomosis of the ovarian pedicle is technically feasible.
In humans, whole fresh ovary was transplanted either orthotopically to the abdomen, with anastomosis of the ovarian artery to the inferior epigastric artery and the ovarian veins to the external iliac vein (16), or heterotopically to the upper arm, with anastomosis of the ovarian artery to the brachial artery and the ovarian veins to the basilic vein (14,15).
In these three cases, the ovary was removed by laparotomy and immediately transplanted by microsurgery. Immediate transplantation is not applicable in patients who need to undergo chemotherapy with highly gonadotoxic agents. In such cases, the ovary needs to be cryopreserved until the patient is in complete remission and wishes to conceive. Successful vascular transplantation of intact frozen-thawed ovaries has been reported in rats (7,8) and sheep (17,18,19,20). In human beings, the main challenge of whole ovary cryopreservation is overcoming the difficulty of adequate cryoprotective agent diffusion into large tissue masses and the risk of vascular injury caused by intravascular ice formation.
However, previous studies in our department (6,21) have demonstrated the feasibility of cryopreservation of intact human ovary with its vascular pedicle using an accessible protocol. We proved high survival rates of follicles, small vessels and stromal cells, as well as a normal histological structure in all ovarian components after thawing (6), and observed no signs of apoptosis or ultrastructural alterations in any cell types (21). Others have also shown maintenance of excellent viability of the superficial and deeper tissue layers of whole human ovaries using a slow-freezing protocol (22).
Vitrification of the ovary is another potential freezing protocol, but it is more difficult to set up (23).
In our opinion, when ovariectomy and whole ovary cryopreservation are performed, two requirements must be met for subsequent transplantation to be feasible. First, the ovarian pedicle must be long enough to allow the ovarian artery and veins to be individualized and sutured to vessels of similar diameter. Second, the ischemic interval before cryopreservation must be as short as possible to avoid damage to the ovary. We believe laparoscopic removal of the ovary fulfills these two conditions.
Laparoscopic dissection of the ovarian pedicle has been performed for a number of years for the purposes of ovarian transposition (24) and is not a difficult procedure for laparoscopic surgeons. The ovarian pedicle can be easily individualized up to the iliac vessels and above the psoas muscle.
The utero-ovarian ligament and the ovarian pedicle may be ligated with sutures. However, because five vascular clips are simpler and faster to place than five sutures, we believe that the use of clips reduces the ischemic interval before ovarian artery perfusion with heparinized solution and cryoprotective medium.
To further reduce the ischemic period, the ovary should be swiftly removed from the abdomen using an endobag, which minimizes damage to the ovary. The endobag should be correctly placed in the abdominal cavity before the ovarian pedicle is clipped. In our view, if all these requirements are met, the duration of ischemia is no longer by laparoscopy than by laparotomy.
Moreover, in patients who need to start chemotherapy as soon as possible, the advantages of laparoscopy over laparotomy (decreased postoperative pain and faster recovery and wound healing) are patently clear.
To keep the time interval between application of the clip to the ovarian pedicle and its perfusion with heparinized solution to an absolute minimum, it is of paramount importance that a microsurgeon and biologist be on hand to immediately dissect the ovarian pedicle and catheterize the ovarian artery. A cooled sterile table equipped with a stereomicroscope and microsurgical instruments must also be within easy reach, and the heparinized solution and cryoprotective medium must be ready for immediate use.
Our studies show that laparoscopic ovariectomy followed by whole ovary cryopreservation is a feasible technique for fertility conservation in women at risk of premature ovarian failure (POF). One must bear in mind, however, that reimplantation of the ovary cannot be considered if there is a risk of neoplastic cell contamination in the ovary. Further studies are also needed to evaluate the risk of thrombosis of the ovarian pedicle after transplantation, as thrombotic events have been reported after autotransplantation of frozen-thawed sheep ovaries (25). We therefore believe that whole ovary cryopreservation should be associated with cryopreservation of heterolateral ovarian cortical biopsies, until the results of ovarian transplantation are validated.
In conclusion, in patients who are at risk of POF, cryopreservation of ovarian tissue should be proposed. Unfortunately, when cortical fragments are cryopreserved, their reimplantation is accompanied by a period of ischemia, causing follicular loss. Vascular transplantation of a whole ovary with its vascular pedicle may well be the solution to this problem.
Removal of an ovary for cryopreservation can easily be achieved by laparoscopy in experienced hands. Care must be taken, however, to secure a long vascular pedicle and to keep the ischemic interval to a minimum.
If these conditions are met, whole ovary cryopreservation and subsequent vascular transplantation could offer hope to countless women in danger of losing their fertility due to gonadotoxic therapy.
Whole ovary transplantation
has the potential to eliminate many of the limitations associated with transplantation of cortical pieces and thus prolong the longevity of the graft.
Objectives
- Review the literature on whole ovary transplantation in the sheep model (26-34)
- Discuss the main technical limitations of the technique
- Discuss potential areas of research
Human ovary transplantation (fresh tissue) has been attempted in the form of heterotopic autotransplants and orthotopic allotransplants. Concerns have been raised about the longevity of grafted ovarian cortical fragments because of the observed fall in the number of primordial follicles due to ischemia. As many as 70% of primordial follicles may be lost to ischemia. Functional vessels are seen from day 7 onwards after transplantation. The concept of whole ovary transplantation arose from the notion that vascular anastomosis would re-establish immediate ovarian perfusion and decrease tissue ischemia.
Sheep have traditionally been used for most experimental studies on ovarian transplantation. The sheep ovary is about 10 mm in diameter, very similar in size to the human ovary. For technical reasons, a heterotopic site was chosen. Our initial experience involved the inferior epigastric vessels, which are easily accessible. Our group showed, with fresh (Jeremias et al, 2002) and frozen (Bedaiwy et al, 2003) whole sheep ovaries, that this approach was technically feasible and able to re-establish normal ovarian function.
Successful autotransplantation of frozen-thawed whole ovary depends on the implementation of:
- A perfusion technique that ensures even and sufficient cryoprotectant permeation of the whole organ, providing the complex organ structure and different cell types with adequate cryoprotection.
- An efficient thawing and perfusion technique that allows effective removal of cryoprotectant.
- An appropriate surgical technique that enables adequate anastomosis and maintains normal reperfusion.
The ovary should be removed in a way that salvages as much of the ovarian vessel as possible. This vessel is used to perfuse the whole ovary, usually with the help of a pump. Whole frozen sheep ovaries fit into routinely used cryochambers, but human ovaries from reproductive-age women do not and therefore require the use of special technology.
Although whole ovary transplantation with vascular anastomosis has been successful in sheep (Revel et al, 2004; Arav et al, 2005; Imhof et al, 2006; Grazul-Bilska A, 2008), a number of worrying observations have emerged.
In Revel’s study:
- Unsuccessful anastomosis was noted in 3/8 sheep; 2 cases of vessel thrombosis
- In 5 cases of successful anastomosis: adhesions in 4/5 sheep
- 3/8 sheep showed normal progesterone activity
In Arav’s study:
- The same sheep population as in Revel’s study
- Progesterone activity noted 36 months after vascular transplantation of frozen-thawed sheep ovaries in 3/8 transplants (only 2 after 24 and 36 months)
- Retrieval of 6 oocytes:
- two sheep yielded one oocyte each
- one sheep yielded 4 oocytes 4 months later
- embryonic development to the 8-cell stage
In Imhof’s study:
- Orthotopic autotransplantation of frozen-thawed whole sheep ovaries with anastomosis to the ovarian vascular pedicle:
- 3/8 cases showed progesterone activity (1 achieved pregnancy) after 1 year
- 4/8 showed no progesterone activity
- 1/8 was euthanized within 2 months
- 1 sheep was euthanized at 2 months (no problems)
- 1 sheep gave birth
- 6 sheep were euthanized 18-19 months after transplantation:
- 4 cases were vascularized and perfused, but showed local damage (30-50% of the ovary)
- Local thrombosis?
– 2 sheep exhibited complete atrophy of the ovaries
- Follicle count approximately 18-19 months after transplantation in 8 sheep = 1-7 % compared with fresh ungrafted ovary
Morphology and function of cryopreserved whole ovine ovaries after heterotopic autotransplantation:
In a study we performed in conjunction with North Dakota State University on heterotopic transplantation of whole ovaries with frozen vascular pedicles, we again noted a high degree of loss (Grazul-Bilska A et al). Only 2 ovaries out of 16 (8 ewes) survived. Follicles were obtained, from which cumulus-oocyte complexes were identified and in vitro matured, but none fertilized. However, the morphology of the autotransplanted ovaries that survived was similar to control ovaries.
Human study
Dr. Silber reported a successful pregnancy after microsurgical transplantation of an intact ovary. The ovarian transplant was a fresh ovary from one twin to another (monozygotic) with premature ovarian failure. The patient established regular periods and achieved pregnancy spontaneously. The report highlights the tough technical nature of transplantation with an ovarian artery of 0.5 mm.
Conclusion
Results from animal studies have highlighted a number of concerns that require more research:
- Ischemia time (from tissue harvesting to freezing, from thawing to completion of anastomosis)
- Reperfusion injury
- Oxidative stress causing premature oocyte senescence
- Damage to vessels secondary to cryopreservation
- Difficulties with freezing techniques
- High level of follicular loss after whole ovary transplantation
- Technical challenges of vascular anastomosis
References :
- Oktay K, Karlikaya G. Ovarian function after transplantation of frozen, banked autologous ovarian tissue. N Engl J Med 2000;342:1919.
- Nisolle M, Casanas-Roux F, Qu J, Motta P, Donnez J. Histologic and ultrastructural evaluation of fresh and frozen-thawed human ovarian xenografts in nude mice. Fertil Steril 2000;74:122-9.
- Baird DT, Webb R, Campbell BK, Harkness LM, Gosden RG. Longterm ovarian function in sheep after ovariectomy and transplantation of autografts stored at -196°C. Endocrinology 1999;140:462-71.
- Kim SS, Yang HW, Kang HG, Lee HH, Lee HC, Ko DS, Gosden RG. Quantitative assessment of ischemic tissue damage in ovarian cortical tissue with or without antioxidant (ascorbic acid) treatment. Fertil Steril 2004;82:679-85.
- Gosden RG, Baird DT, Wade JC, Webb R. Restoration of fertility to oophorectomized sheep by ovarian autografts stored at -196 degrees C. Hum Reprod 1994;9:597- 603.
- Martinez-Madrid B, Dolmans MM, Van Langendonckt A, Defrere S, Donnez J. Freeze-thawing intact human ovary with its vascular pedicle with a passive cooling device. Fertil Steril 2004;82:1390-4.
- Wang X, Chen H, Yin H, Kim SS, Tan SL, Gosden RG. Fertility after intact ovary transplantation. Nature 2002;415:385.
- Yin H, Wang X, Kim SS, Chen H, Tan SL, Gosden RG. Transplantation of intact rat gonads using vascular anastomosis: effects of cryopreservation, ischemia and genotype. Hum Reprod 2003;18:1165-72.
- Jeremias E, Bedaiwy MA, Gurunluoglu R, Biscotti CV, Siemionow M, Falcone T. Heterotopic autotransplantation of the ovary with microvascular anastomosis: a novel surgical technique. Fertil Steril 2002;77: 1278-82.
- Goding JR, McCracken JA, Baird DT. The study of ovarian function in the ewe by means of a vascular autotransplantation technique. J Endocrinol 1967;39:37-52.
- Winston RM, Browne JC. Pregnancy following autograft transplantation of Fallopian tube and ovary in the rabbit. Lancet 1974;2:494 -5.
- Paldi E, Gal D, Barzilai A, Hampel N, Malberger E. Genital organs. Auto and homotransplantations in forty dogs. Int J Fertil 1975;20:5-12.
- Scott JR, Keye WR, Poulson AM, Reynolds WA. Microsurgical ovarian transposition in the primate. Fertil Steril 1981;36:512-5.
- Leporrier M, von Theobald P, Roffe JL, Muller G. A new technique to protect ovarian function before pelvic irradiation. Heterotopic ovarian autotransplantation. Cancer 1987;60:2201- 4.
- Hilders CG, Baranski AG, Peters L, Ramkhelawan A, Trimbos JB. Successful human ovarian autotransplantation to the upper arm. Cancer 2004;101:277-8.
- Mhatre P, Mhatre J, Magotra R. Ovarian transplant: a new frontier. Transplant Proc 2005;37:1396-8.
- Bedaiwy MA, Jeremias E, Gurunluoglu R, Hussein MR, Siemianow M, Biscotti C, et al. Restoration of ovarian function after autotransplantation of intact frozen-thawed sheep ovaries with microvascular anastomosis.Fertil Steril 2003;79:594-602.
- Revel A, Elami A, Bor A, Yavin S, Natan Y, Arav A. Whole sheep ovary cryopreservation and transplantation. Fertil Steril 2004;82: 1714-5.
- Arav A, Revel A, Nathan Y, Bor A, Gacitua H, Yavin S, et al. Oocyte recovery, embryo development and ovarian function after cryopreservation and transplantation of whole sheep ovary. Hum Reprod 2005; 20:3554-9.
- Imhof M, Bergmeister H, Lipovac M, Rudas M, Hofstetter G, Huber J. Orthotopic microvascular reanastomosis of whole cryopreserved ovine ovaries resulting in pregnancy and live birth. Fertil Steril. 2006 Apr;85 Suppl 1:1208-15.
- Martinez-Madrid B, Camboni A, Dolmans MM, Nottola SA, Van Langendonckt A, Donnez J. Apoptosis and ultrastructure in frozen intact human ovary. Hum Reprod 2005;20(Suppl 1):i37-8.22. Bedaiwy MA, Hussein MR, Biscotti C, Falcone T. Cryopreservation of intact human ovary with its vascular pedicle. Hum Reprod. 2006;21(12):3258-69.
- Bedaiwy MA, Hussein MR, Biscotti C, Falcone T. Cryopreservation of intact human ovary with its vascular pedicle. Hum Reprod. 2006;21(12):3258-69.
- Courbiere B, Caquant L, Mazoyer C, Franck M, Lornage J, Salle B. Difficulties improving ovarian functional recovery by microvascular transplantation and whole ovary vitrification. Fertil Steril. 2009 Jun;91(6):2697-706.
- Nisolle M, Squifflet J, Donnez J. Laparoscopic ovarian transposition. In: Donnez J, Nisolle M, eds. An atlas of operative laparoscopy and hysteroscopy. Carnforth, Lancs, UK; Parthenon, 2001:331-4.
- Bedaiwy MA, Falcone T. Ovarian tissue banking for cancer patients.Reduction of post-transplantation ischaemic injury: intact ovary freezing and transplantation. Hum Reprod 2004;19:1242-4.
- Arav A, Revel A, Nathan Y, Bor A, Gacitua H, Yavin S, Gavish Z, Uri M, Elami A. Oocyte recovery, embryo development and ovarian function after cryopreservation and transplantation of whole sheep ovary. Hum Reprod 2005; 20(12):3554-9.
- Bedaiwy MA, Jeremias E, Gurunluoglu R, Hussein M, Biscotti C, Siemionow M, Falcone T. Transplantation of intact frozen-thawed mammalian ovary with vascular anastomosis. Fertil Steril 2003; 79:594-602.
- Grazul-Bilska A, Banerjee J, Yazici I, Borowczyk E, Bilski J, Sharma R, Siemionov M, Falcone T. Morphology and function of cryopreserved whole ovine ovaries after heterotopic autotransplantation. Reprod Biol Endocrinol 2008. In press.
- Imhof M, Bergmeister H, Lipovac M, Rudas M, Hofstetter G, Huber J. Orthotopic microvascular reanastomosis of whole cryopreserved ovine ovaries resulting in pregnancy and live birth. Fertil Steril 2006; 85:1208-1215.
- Jeremias E, Bedaiwy MA, Gurunluoglu R, Biscotti CV, Siemionow M, Falcone T. Heterotopic autotransplantation and vascular anastomosis: a novel surgical technique. Fert Steril 2002; 77:1278-82.
- Revel A, Elami A, Bor A, Yavin S, Natan Y, Arav A. Whole sheep ovary cryopreservation and transplantation. Fertil Steril 2004; 82(6):1714-5.
- Courbiere B, Odagescu V, Baudot A, Massardier J, Mazoyer C, Bruno S, Lornage J. Cryopreservation of the ovary by vitrification as an alternative to slow-cooling protocols. Fertil Steril 2006;86sup:1243-1251.
- Grazul-Bilska A, Banerjee J, Yazici I, Borowczyk E, Bilski J, Sharma R, Siemionov M, Falcone T. Morphology and function of cryopreserved whole ovine ovaries after heterotopic autotransplantation. Reprod Biol Endocrinol 2008; 6:16-32.
- Silber S, Grudzinskas G, Gosden R. Successful pregnancy after microsurgical transplantation of an intact ovary. N Engl J Med 2008;359;2617-2618.